
In the previous section, we have mentioned that Energy Expenditure (EE) may help to identify inactive lifestyles and to promote towards a more active lifestyle. Indeed, there are direct methods of EE measurement but they are uncomfortable for patient during daily life activities. So, the estimation of EE (in MET or kcal/h) from respiratory signals and Breathing Rate (BR) constitutes original approaches more wearable and less cumbersome; and complementary information to existing signals such as heart rate and acceleration signal. While direct methods exist for measuring respiratory rate, they usually requires specific equipment not comfortable for patient. The electrocardiogram (ECG) contains information about the respiratory rate and are known as indirect measurements to extract breathing rate.
Database
Our study was done in a dataset covering activities of daily living: sitting, standing, lying, working on pc, rinding a car, walking, with each activity duration for at least 6 min. A continuous ECG signal is collected at 250 Hz using Zephyr sensor and simultaneously a respiratory rate is obtained from a nasal airflow cosmed sensor (k4B2).
Methods
We are aiming to obtain precise information as direct measurement of respiratory devices are uncomfortable during daily activities. This estimation is based on 4 EDRs modulations: EDR R apmlitude, QR amplitude, QRS area and RSA extracted from ECg signal. Due to the noisy and patient dependence nature of the EDR signals, it is difficult to determine the combination of EDR modulations that best adapts to activity intensities and patient specificities to yield the best BR estimation performances. Hence, we propose a solution by using respiratory quality indices (RQI) to quantify the quality of respiratory signal information before estimation of breathing rate. We developed two approaches to estimate BR. The first approach consists of an automatic selection of the most relevant EDR with highest RQI, from the 4 derived modulations. In the second method a fusion algorithm using Kalman Smoother (KS) with two EDR inputs (of the higest RQI) is proposed to track the respiration signal (see Figure.1).
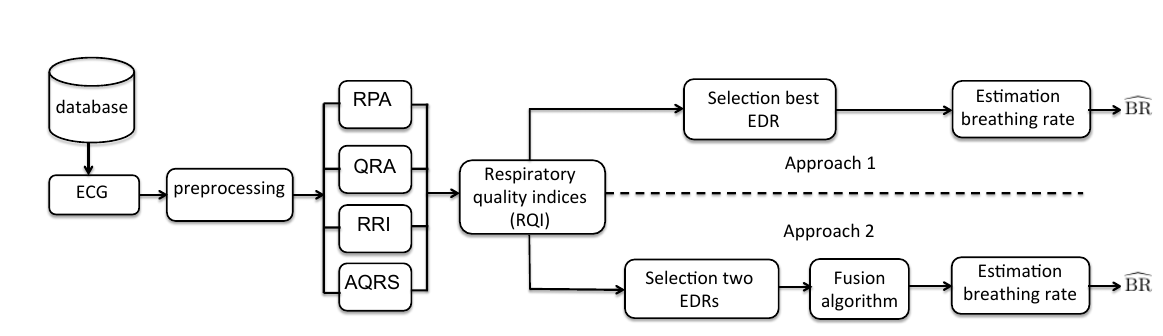
Figure 1: general bloc diagram for the two proposed approach
Some Results…
Table 1 reports the absolute error between the estimated breathing rate from each type of EDRs modulations (EDR RPA, RSA, AQRS and QRA area) and the reference BR. Clearly, the results was improved when we applied fusion algorithm. The improvement was more significant in supine position, car riding and walking activities, where the results was very similar to the manual selection with median absolute error of 1.09 bpm, 1.51 and 2.6 bpm respectively (referred table 1).
